Postpartum
The Struggle: Part II: Why 35% of U.S. Counties Are Now Maternity Care Deserts
Nearly 7 million women of childbearing age live in areas with no or limited access to comprehensive maternity care.

Ilana Shein, MD

Imagine being four months pregnant. You live in a small town in rural America where community ties are strong, but essential services are vanishing.
You feel an unusual twinge, have questions on your mediation or nutrition status, or perhaps you have questions on your risk for gestational and want to look into screening. In an ideal scenario, your OB-GYN or provider is a 15-minute drive away.
For millions of American women, that scenario is a fantasy. Instead, they face a 90-minute drive, each way, sometimes across state lines, just to get their blood pressure checked. This is the reality of America’s “maternity care deserts”—a quiet crisis creating a dangerous geography of inequality where a woman’s zip code determines her likelihood of a healthy pregnancy.
Defining the Desert: The Hard Data
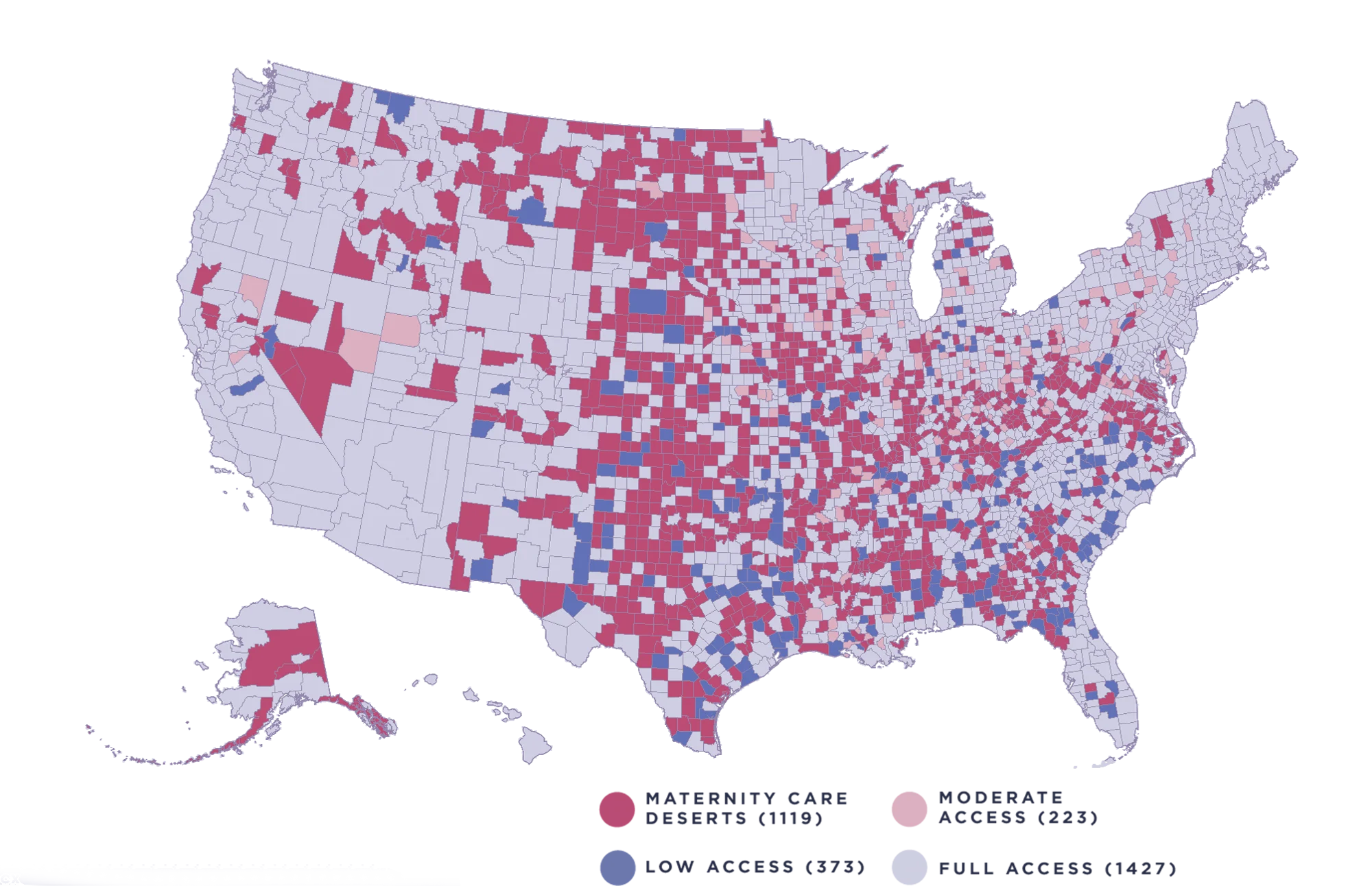
The term "maternity care desert" is a specific designation used to identify areas with zero access to comprehensive obstetric care. The data is sobering.
According to the March of Dimes 2023 Report, more than 36% of all U.S. counties are designated as maternity care deserts. In these counties, there are:
Zero hospitals providing obstetric care.
Zero birth centers.
Zero OB-GYNs or certified nurse-midwives.
Nearly 7 million women of childbearing age live in areas with no or limited access to comprehensive maternity care. The trend is moving in the wrong direction: between 2020 and 2022, over 100 counties shifted from having "some access" to becoming full deserts.
The Prenatal Burden: The "Windshield Time" Penalty
The immediate consequence of living in a care desert is the immense amount of time spent driving. While urban residents may travel 10–20 minutes to a clinic, the Government Accountability Office (GAO) reports that rural residents often travel twice as far. In deep deserts, it is not uncommon for women to drive two hours one-way for a 15-minute checkup.
When the barriers—gas money, time off work, and childcare—become too high, care is often delayed or skipped. The CDC notes that women who receive no prenatal care are three to four times more likely to die from pregnancy-related complications.
The "Danger Zone": The Postpartum Crisis
The crisis doesn't end at delivery. The "fourth trimester" (the weeks following birth) is actually the most dangerous time for a new mother.
Data from the CDC reveals that more than 52% of pregnancy-related deaths occur after the day of delivery.
1–6 days postpartum: 14% of deaths.
7–42 days postpartum: 18% of deaths.
43 days to 1 year postpartum: 20% of deaths.
In a care desert, a woman experiencing delayed-onset preeclampsia or a post-surgical infection is hours away from help. The "windshield time" that was a nuisance during pregnancy becomes a life-threatening barrier during a postpartum emergency.
The Invisible Toll: Mental Health and Isolation
Perhaps the most overlooked consequence is the impact on maternal mental health. The Policy Center for Maternal Mental Health identifies mental health conditions (including suicide and overdose) as the leading cause of pregnancy-related deaths in the U.S., accounting for roughly 23% of cases.
In maternity deserts, these risks are amplified:
Higher Prevalence: Postpartum depression (PPD) rates in rural women can reach 32%, significantly higher than the national average.
Specialist Scarcity: Many desert counties have zero psychiatrists or specialized counselors within a 100-mile radius.
Profound Isolation: The physical distance from providers exacerbates the "baby blues" into deep clinical depression because there is no local safety net to catch the fall.
Bridging the Gap: The Role of Virtual Care
The physical infrastructure for maternity care is crumbling, and rebuilding brick-and-mortar hospitals in every county is a long-term project. However, pregnant and postpartum women need help today. This is where virtual care and telehealth models, such as Phia Health (www.phiahealth.com), are stepping in as a clinical lifeline.
Virtual care models are shifting the paradigm from "geographic-dependent" care to "patient-centered" care:Remote Patient Monitoring (RPM): Using connected devices (like blood pressure cuffs) at home allows providers to track signs of preeclampsia in real-time, replacing a four-hour round trip with a digital check-in.
Mental Health Integration: Digital platforms can deploy frequent screenings (like the Edinburgh Postnatal Depression Scale) to catch PPD early and provide instant video access to specialized counselors.
Lactation and Triage Support: Virtual consultations can determine if a postpartum symptom requires an emergency room visit or can be managed at home, saving precious time and resources.
The Bottom Line
Living in a "desert" should not mean being left alone. While we must advocate for better rural hospital funding, we must also embrace technology that brings expertise directly into the home. By leveraging platforms like Phia Health, we can begin to shrink the distances that separate millions of American mothers from the care they need to survive and thrive.
How designers estimate the impact of UX?
The Struggle: Part II: Why 35% of U.S. Counties Are Now Maternity Care Deserts
The Struggle: Part II: Why 35% of U.S. Counties Are Now Maternity Care Deserts
Nearly 7 million women of childbearing age live in areas with no or limited access to comprehensive maternity care.
Nearly 7 million women of childbearing age live in areas with no or limited access to comprehensive maternity care.
Ilana Shein, MD
Published in Fintech
Postpartum
Image credit by Yum Yum
Imagine being four months pregnant. You live in a small town in rural America where community ties are strong, but essential services are vanishing.
You feel an unusual twinge, have questions on your mediation or nutrition status, or perhaps you have questions on your risk for gestational and want to look into screening. In an ideal scenario, your OB-GYN or provider is a 15-minute drive away.
For millions of American women, that scenario is a fantasy. Instead, they face a 90-minute drive, each way, sometimes across state lines, just to get their blood pressure checked. This is the reality of America’s “maternity care deserts”—a quiet crisis creating a dangerous geography of inequality where a woman’s zip code determines her likelihood of a healthy pregnancy.
Defining the Desert: The Hard Data
The term "maternity care desert" is a specific designation used to identify areas with zero access to comprehensive obstetric care. The data is sobering.
According to the March of Dimes 2023 Report, more than 36% of all U.S. counties are designated as maternity care deserts. In these counties, there are:
Zero hospitals providing obstetric care.
Zero birth centers.
Zero OB-GYNs or certified nurse-midwives.
Nearly 7 million women of childbearing age live in areas with no or limited access to comprehensive maternity care. The trend is moving in the wrong direction: between 2020 and 2022, over 100 counties shifted from having "some access" to becoming full deserts.
The Prenatal Burden: The "Windshield Time" Penalty
The immediate consequence of living in a care desert is the immense amount of time spent driving. While urban residents may travel 10–20 minutes to a clinic, the Government Accountability Office (GAO) reports that rural residents often travel twice as far. In deep deserts, it is not uncommon for women to drive two hours one-way for a 15-minute checkup.
When the barriers—gas money, time off work, and childcare—become too high, care is often delayed or skipped. The CDC notes that women who receive no prenatal care are three to four times more likely to die from pregnancy-related complications.
The "Danger Zone": The Postpartum Crisis
The crisis doesn't end at delivery. The "fourth trimester" (the weeks following birth) is actually the most dangerous time for a new mother.
Data from the CDC reveals that more than 52% of pregnancy-related deaths occur after the day of delivery.
1–6 days postpartum: 14% of deaths.
7–42 days postpartum: 18% of deaths.
43 days to 1 year postpartum: 20% of deaths.
In a care desert, a woman experiencing delayed-onset preeclampsia or a post-surgical infection is hours away from help. The "windshield time" that was a nuisance during pregnancy becomes a life-threatening barrier during a postpartum emergency.
The Invisible Toll: Mental Health and Isolation
Perhaps the most overlooked consequence is the impact on maternal mental health. The Policy Center for Maternal Mental Health identifies mental health conditions (including suicide and overdose) as the leading cause of pregnancy-related deaths in the U.S., accounting for roughly 23% of cases.
In maternity deserts, these risks are amplified:
Higher Prevalence: Postpartum depression (PPD) rates in rural women can reach 32%, significantly higher than the national average.
Specialist Scarcity: Many desert counties have zero psychiatrists or specialized counselors within a 100-mile radius.
Profound Isolation: The physical distance from providers exacerbates the "baby blues" into deep clinical depression because there is no local safety net to catch the fall.
Bridging the Gap: The Role of Virtual Care
The physical infrastructure for maternity care is crumbling, and rebuilding brick-and-mortar hospitals in every county is a long-term project. However, pregnant and postpartum women need help today. This is where virtual care and telehealth models, such as Phia Health (www.phiahealth.com), are stepping in as a clinical lifeline.
Virtual care models are shifting the paradigm from "geographic-dependent" care to "patient-centered" care:Remote Patient Monitoring (RPM): Using connected devices (like blood pressure cuffs) at home allows providers to track signs of preeclampsia in real-time, replacing a four-hour round trip with a digital check-in.
Mental Health Integration: Digital platforms can deploy frequent screenings (like the Edinburgh Postnatal Depression Scale) to catch PPD early and provide instant video access to specialized counselors.
Lactation and Triage Support: Virtual consultations can determine if a postpartum symptom requires an emergency room visit or can be managed at home, saving precious time and resources.
The Bottom Line
Living in a "desert" should not mean being left alone. While we must advocate for better rural hospital funding, we must also embrace technology that brings expertise directly into the home. By leveraging platforms like Phia Health, we can begin to shrink the distances that separate millions of American mothers from the care they need to survive and thrive.

Let’s talk about your members.
Let’s talk about your members.
A 30-minute capabilities briefing walks through the care model, how a partnership operates in practice, and a population-specific impact estimate built on your gap data.